




PATHOGENESIS
Renal tuberculosis occurs by infectious agents diffusing from infected lungs or hilar lymph nodes (regional lymph nodes between the lungs) into both kidneys via bloodstream.
Diseases occur by reactivation of dormant bacilli in the cases such as general status disorder, trauma, steroid treatment, diabetes, anemia, immunosupression and AIDS (acquired immunodeficiency syndrome).
Bacilli pass into the ureter and then bladder by the urine as they damage the inner structure of the kidney. During this pass, they cause development of strictures on ureters, bladder inflammation and contracture. Local injuries occurred at the beginning combine by time and may damage to the kidney completely and putty kidney occurs. Infected urine passage in the urogenital tract may cause ureter, bladder, prostate, seminal vesicles, vas deference, epididym and testicle involvement. However, lesions may also occur by primary hematogenous dissemination in the prostate.
CLINICAL PICTURE AND DIAGNOSIS
Renal tuberculosis occurs by infectious agents diffusing from infected lungs or hilar lymph nodes (regional lymph nodes between the lungs) into both kidneys via bloodstream.
Diseases occur by reactivation of dormant bacilli in the cases such as general status disorder, trauma, steroid treatment, diabetes, anemia, immunosupression and AIDS (acquired immunodeficiency syndrome).
Bacilli pass into the ureter and then bladder by the urine as they damage the inner structure of the kidney. During this pass, they cause development of strictures on ureters, bladder inflammation and contracture. Local injuries occurred at the beginning combine by time and may damage to the kidney completely and putty kidney occurs. Infected urine passage in the urogenital tract may cause ureter, bladder, prostate, seminal vesicles, vas deference, epididym and testicle involvement. However, lesions may also occur by primary hematogenous dissemination in the prostate.
CLINICAL PICTURE AND DIAGNOSIS Genital tuberculosis is a slow progressing disease and appears at 15 to 20 years after the primary pulmonary infection in general. This period may extend to 35 years or more. It is as twice as frequent in men. 80% of the patients are symptomatic during the diagnosis.
Pollakiuria (frequent urination), urgency (urgent urination desire), nocturia (awakening for urination at night), dysuria (burning sense while urinating) may be detected. 50% of the patients have macroscopic hematuria (visual urinary bleeding). These symptoms may not be seen until the disease progresses to the further stage; even though patients may be asymptomatic. Pain is an indicator for a progressed disease. Most symptoms are connected with dissemination of the bacilli into the bladder.
Physical examination may not provide much information about the disease progress. If vas deference is involved, they are nodular or like rosary beads. Prostate and epididymis may be hard and nodular.
Unless bilateral involvement occurs, renal function is normal. In urine analysis of 90% of the patients, erythrocytes, leukocytes and acidic pH are detected. Although reproduction is not detected in routine cultures, superinfections which include E. coli in general may be present by 20%.
A specific culture should be performed for mycobacterium from the first urine of the patient in the morning. The ratio of a single culture to be positive is 73%. By the specific cultures performed with the first urine for 3 subsequent days, achievement rate may be increased to 90%. No better results have been obtained on tests performed by collecting 24 hours urine. Also, acid resistant bacillus may be investigated by staining the first urine n the morning with Ziehl-Neelsen, Kinyoun or fluorochrome for subsequent 3 days. The PCR (polymerase chain reaction) which has improved fast recently is very safe and fast method in the diagnosis.
PPD Skin test may be non-reactive in 15% of the patients with genitourinary tuberculosis. Pulmonary disease is not detected in lung radiographies of 20 to 50% of the patients.
The standard test for the diagnosis is intravenous pyelography (IVP) and provides an abnormal findings in 93% of the patients.
Poor calcifications on tuberculoms may be detected on direct radiography.
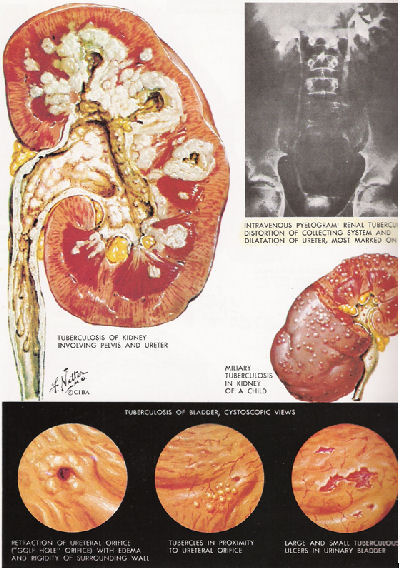
In contrast graphs, stenosis, dilatations and parenchyma disruptions are detected in collecting systems. It causes autonephrectomy, namely complete function loss of the kidney at the late term. Changes on ureter appears as single or multiple stenosis, dilatation, beading or corkscrew. Bladder may be small and contracted. Antegrade or retrograde pyelography may be applied to view non-functioning kidneys.
Ulcer and nodules which have generally located around ureter orifices and are smaller than 3 mm may be detected in the cystoscopy. Orifices may be abnormal; bladder mucosa may be inflammatous and edematous diffusely.
After the urinary system, prostate, seminal vesicles, epididyms and testicles may be involved by a gradually reduced ratios. Galling fistula in the scrotum is another finding for the tuberculosis. Urethra involvement is rare and may be shown with voiding cystourethrography. Penile tuberculosis is in the form of superficial ulcer, but it may involve the tissues below. The diagnosis should be established by a biopsy to discard the malignancy possibility. Lesions on female reproductive organs may cause ectopic pregnancy or sterility.
Some Clinical Findings For Genitourinary Tuberculosis
- Sterile pyuria
- Painless and frequent urination at nights
- Previous or active tuberculosis on another part of the body
- Unexplained hematuria
- Chronic cystitis irresponsive to antibiotics
- Chronic epididymitis including nodules in the epididymis and/or thick ductus deference or palpation of formations like rosary beads
- Waned nodular prostate
- Indurations on seminal vesicles
- Mild iliac pain / renal colic
- Scrotal sinuses including chronic efflux
Differential Diagnosis
a– Chronic, nonspecific cystitis or pyelonephritis
b– Acute or chronic nonspecific epididymitis
c– Urethral syndrome, interstitial cystitis
d– Necrotizing papillitis on one kidney or both kidneys
e– Schistosomiasis
Complications
Perinephric abscess or lumbar fistula may develop by dissemination of the renal tuberculosis into the perinephric area. Hydronephrosis and non-functioning kidney (autonephrectomy) picture at last may appear because of ureter stenosis. Bilateral kidney involvement and chronic kidney failure may develop at the advanced stage. Sometimes, kidney stones secondary to the infection may be detected. If the bladder is involved, low capacity contracted bladder may occur in time. Infertility may develop due to the obstruction on epididymis or ductus deference involvement as well as chronic fistulas are frequent.
TREATMENT
1- General Considerations
The main purpose of the anti-tuberculosis treatment is to treat the active disease fast and put the disease into a non-active period within a short time period. Several synergistic drugs are used together to prevent resistant microorganism formation at the early period of the disease. While using such drugs, urethral stenosis as 1/3 distal part of the ureter in particular may appear within the recovery period. Tuberculosis strictures are susceptible for percutaneous or transurethral dilatation techniques. Surgical intervention may be required for genitourinary tuberculosis cases which present progression trend within a short period against antibiotic therapy.
2 – Standart Tedavi
One of the problematic subjects of the treatment is what the period should be. Previously, medical therapy has been given for 2 years at least. In 1980s, triple or quadruple combination regimens have been recommended for pulmonary tuberculosis for 6 to 9 months. Some physicians apply these short term therapies for genitourinary tuberculosis as well. The logic for this is that drugs can reach to high concentrations in renal parenchyma and other parts of the urinary system, they are discharged by the urine and bacterial count on genitourinary tuberculosis is less than those in pulmonary infection. Another group suggests that a therapy for 9 months is very short and a therapy for 1 to 3 years is required. The problem for long term therapy is patient incompliance with a high ratio and drug side effects. Triple or quadruple combination is applied for the first 2 to 3 months and then maintenance therapy is applied with 2 agents in both therapy regimens.
Drugs used in the treatment may be grouped under 3 main groups:
1– Primary agents: They have a bactericide effect. This group includes rifampicin, isoniazid (INH), pyrazinamide and streptomycin.
2– Secondary agents: They have a bacteriostatic effect. This group includes ethambutol, ethionamide, cycloserine
And viomycin.
3– Minor agents: The bacteriostatic drugs in this group are kanamycin and thiocetazone.
The therapy may be started with either isoniazid, rifampicin, ethambutol or isoniazid, rifampicin, pyrazinamide or isoniazid, rifampicin, pyrazinamide, streptomycin combinations and isoniazide and rifampicin combination may be used for maintenance. If resistance develops against one of the drugs during the therapy, it is replaced with another drug within the same group. Average adult doses for these agents is provided as follows:
Isoniazid (INH): 300 mg/day, single dose, oral
Ethambutol: 1,200 mg/day, single dose, oral
Rifampin: 600 mg/day, single dose, oral
Streptomycin: 1g/day, single dose, IM.
Pyrazinamide 1.5 to 2 g/day, single dose, oral
Characteristics of antituberculosis drugs are presented in the table. Addition of vitamins B6 and C into the treatment regimens should not be forgotten.
3- Short and Fast Therapy
In this therapy form which has been popularized in UK, the therapy period is 4 months.
– Pyrazinamide 25 mg/kg/gün, günlük doz en fazla 2 gr olmak üzere 4 ay.
– INH, 300 mg/day for 2 months.
– Rifampicin 450 mg/day for 2 months or 900 mg/day for 3 times a week for 2 months.
Medical treatment should be continued for a sufficient period. Surgical treatment is applied as well, if necessary. If any indication appears for surgical treatment, this may be applied at 4 to 6 weeks after initiation of the antibiotherapy. Drain placement in case of perinephric abscess; if non-functioning kidney or persistent pain, bleeding, hypertension, bacterial persistence are present, nephrectomy; open or closed surgical interventions for urethral stenosis; and augmentation cystoplasty for severe bladder contractures (surgical interventions to increase the bladder capacity) may be applied. If tuberculosis dependent orchitis and epididymitis do not respond to the treatment or they are fistulized into the scrotum, epididymectomy or orchiectomy may be necessary.
Monitoring
The patients should be examined at 3rd, 6th and 12th months after completion of the treatment, urine cultures should be done and acidoresistant bacteria should be searched. Kidneys, ureters and bladder are examined with radiographic studies.