




GHONORRHEA: GONOCOCCAL URETHRITIS
The cause for gonococcal urethritis is Neisseria gonorrhea, a gram negative diplococcus. Although incubation period varies between 3 and 10 days, the period required for development of symptoms may be as short as 12 hours or as long as 3 months.
The most common cause for gonococcal urethritis is sexual intercourse. For a man, infection risk after a single intercourse with an infected partner is about 17 to 20% although the possibility of infection from an infected men to a woman is 80%. When number of sexual intercourse with a porter or infected partner increases, risk also increases. Cases infected with secretions without vaginal intercourse have been reported as well.
SYMPTOMS AND FINDINGS
- Burning sense while urinating
- Urethral efflux (Efflux is generally inflamed, yellow to brown colored and much)


DIAGNOSIS
Gram staining and planting into the culture medium from samples are performed. 2 separate samples are collected if necessary. Gram-negative diplococcus are seedn in the gram staining. An accurate diagnosis may be determined with 95%.
COMPLICATIONS
Periurethritis, periurethral abscess
Urethral stenosis
Prostatitis, prostate abscess, epididymitis, proctatitis and arthritis may be seen.
PROTECTION
Gonorrhea may be prevented with regular condom use and antibiotic after the intercourse, intravaginal antiseptic agents or antibiotic application. Ceftriaxone, Spectinomycin Ciprofloxacin ,Norfloxacin , Cefuroxime axetil, Ceftizoksime and Amoxicillin may be used fort he treatment. Patient monitoring after the treatment is important. If urethritis continues at 3rd to 7th day of the treatment, resistance, post gonococcal urethritis or re-infection should be considered.
NON-GONOCOCCAL URETHRITIS (NGU)
When N. gonorrhea can not be shown by the culture or gram staining in presence of urethritis, non-gonococcal urethritis is diagnosed. The most important and dangerous cause is Chlamydia trachomatis. This bacteria may be shown in 25 to 60% of men with NGU and 4 to 35% of men with gonorrhea in urethra. There is not any pathology ,n 50% of Chlamydia infections, but patients are porter. In 20 to 50% of the patients, the cause for NGU is Ureaplasma urealyticum. It is most common between 20 and 24 years of life. 50 to 75% of acute urethritis are non-gonococcal. Incubation period varies between 7 and 35 days.
Symptoms :
- Urethral efflux (efflux is generally less, thin and mucoid)
- Dysuria (burning sense while urinating) and urethral itching and stinging sense.
For NGU diagnosis, N. gonorrhoeae should be discarded with gram staining and culture when urethritis is present. The most ideal in gram staining is to apply the procedure on the sample taken at 4th hour after the urination.
TREATMENT
Tetracycline, doxycycline or erythromycin may be used. To be protected from NGU is limited with condom like in gonorrhea and vaginal spermicidal agents. Treatment of the patient with her/his sexual partners are very important.
SYPHILIS
Syphilis is caused by a spirochete called Treponema pallidum. T. pallidum enters into the body by skin and mucosa and a painless chancre ( a wound seems like a hole made by a staple) on the penis at 2 to 4 weeks after the sexual intercourse. Pain is not detected with pressure. If not treated, lesion recovers slowly by itself. The disease passes into the 2nd phase. There may be unilateral or bilateral, separate, painless lymphadenopathy on the inguinal region.

LABORATORY FINDINGS
It is diagnosed with observing the spirochetes by performing a dark field examination on the material obtained by scratching the chancre base or by fluorescent antibody techniques. If dark field examination can not be applied, serological tests should be used. Serological tests may be negative even at 1 to 3 weeks after appearance of the chancre.
COMPLICATIONS
Urological complications are rare and seen at the 3rd phase of the disease. These include testicle gummas and neurogenic bladder seen in neurosyphilis.
TREATMENT
Penicillin G is given to the patients with early syphilis. Doxycycline or tetracycline is given to those with penicillin allergy.
The illustration shows a syphilis dependent wound on the penis
TRICHOMONIASIS
Trichomonas vaginalis causes the disease. Incidence is 2%. T is most common between 15 and 40 years of life in men and women. It spreads with sexual intercourse and it was found with a ratio of 14 to 60% in male partners of infected women and of 67 to 100% in female partners of infected men. It mostly progresses without any symptom in men.
Urethral efflux is just mixed with 1 to 2 ml physiological saline and examined microscopically. Although precision of this examination in women is 60 to 70%, safety is less in men.
TREATMENT
Condom should be used until the treatment is completed successfully. Metronidazole is given to the patient and her partner. Treatment response is taken immediately. Treatment of partners earnestly is very important.
CHANCROID (ULCUS MOLLE, SOFT CHANCRE)
It is caused by Haemophilus ducreyi.
The first symptom of chancroid is the papule seen on several days after the sexual intercourse. Then, single or multiple, painful chancroid ulcers with a dirty appearance appear. They cause inflamed efflux in general. The patients have fever, headache and fatigue.
Ulcers not treated grow slowly, bursts and combine with the others. It causes painful groin inflammation and lymphatic obstruction; and genital edema and further elephantiasis develop.
Gram-negative coccobacillus are seen in gram staining examination of the sample taken from the ulcer in 50% of the patients. Biopsy is always diagnostic.
TREATMENT
Azithromycin 1 g. Single dose, erythromycin 500 mg. For 4 x 17 days, certraixone 250 mg may be used as single dose. HIV test during the diagnosis and after 3 months are appropriate. Prognosis is very well with an appropriate treatment.
LYMPHOGRANULOMA VENEREUM
The cause is Chlamdyda Trachomatis. Genital lesion, lymphadenitis and rectal stenosis may be seen. A papule or pustule appears at 5 to 21 days after the sexual intercourse. Genital lesion is small and generally not noticed. Reproduction of C. trachomatis in the culture is diagnostic.
COMPLICATIONS
Galling sinuses occur by rupture of the inguinal lymph nodes. Chronic inguinal inflammation may cause lymphatic obstruction and elephantiasis. Rectal stenosis is a late complication.
TREATMENT
Doxycycline, 100 mg. 2×1, for 3 weeks.
GRANULOMA INGUINALE
The cause is Calymmatobacterium granulomatis (Donovan body) and incubation period is 2 to 3 months.
CLINICAL FINDINGS
Papule is the first symptom. A painless, tumorous, hard, indurated, painless ulcer including hemorrhagic secretion with an eritematous base occurs. Observation of Donovan bodies in stained smear is diagnostic.
TREATMENT
Tetracycline 500 mg. 4×1 or trimethoprim-sulfamethoxazole (160/800 mg. tablet) 2×1 are applied until the lesions recover.
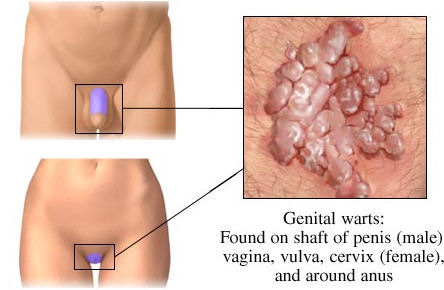
CONDILOMA ACUMINATA (WART)
The cause is HPV (Human papilloma virus). Incubation period may be 1 to 2 months. Diagnosis is very easy by observing the lesion.
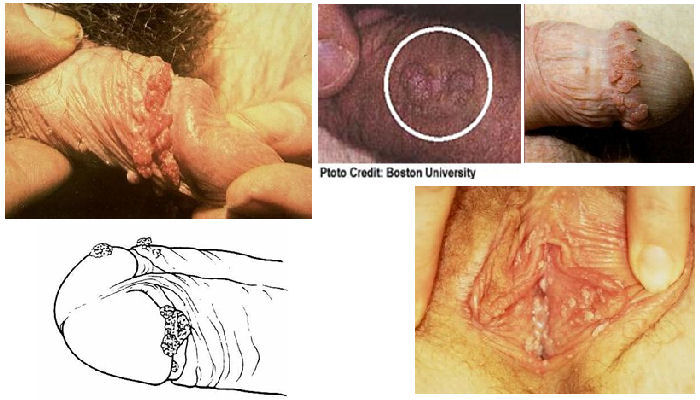
Location, size and number of the lesions are important for the treatment.
Topical creams: Podophylin – imiquimod cream, trichloracetic acid may be used.
Cryotherapy: Lesions may be destroyed without pain within a couple of sessions.
Surgical: Removal of the lesions completely one by one and cauterization of the wart base is the most efficient therapy. It may be applied in the office under local anesthesia.
* It is possible to cauterize urethral warts endoscopically.