




DEFINITION OF ERECTILE DYSFUNCTION (ED)
Inability to provide and maintain required and sufficient erection for a sexual intercourse.
- ED is an important health problem.
- There are 30 million men with ED in USA
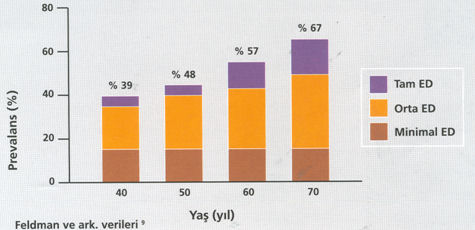
- This problem is present in 70% of men over 40 years in Turkey with different aspects
- Effect of ED to social life is very important
- The patients do not consult with a physician or delay on consulting because of sexual taboos.
- Low diagnosis rates for erectile dysfunction depend on insufficient communication between the Physician and the Patient.
- Only 10% of men with ED between 18 and 60 years refer to a physician by suggesting this complaint!

Physicians may also have prejudices about ED;
- They assume that sexual issues are out of professionalism
- They think that this damages to the relation with the patient.
- The concern about attacking private life
- Hesitation to shame the patient
- Not having time to allocate for this subject causes delays on diagnosis and treatment.
Permanent problem under 40 years: Rare
70 years and over : % 65
* Complaints start earlier in diabetic patients!!!
CAUSES FOR ED
- ORGANIC
Vascular – Neurological – Hormonal – Due to disorders of the penis nature
- PSYCHOGENIC
Suppression of the erectile mechanism by the brain without any physical disorder.
However, many patients have Organic + Psychogenic problems together.
Psychological Vascular Neurogenic Hormonal Drugs
Anxiety Atherosclerosis Trauma Androgen deficiency Anxiolytic drugs
Depression Hyperlipidemia Surgical Hyperprolactinemia Antidepressants
Intercourse problems Smoking MULTIPLE SCLEROSIS Thyroid diseases Antihypertensives
Diabetes Herniated disc Antiandrogenic drugs
Hypertension Diabetes Digoxin
Alcohol Cimetidine
Most common findings in men with ED
Hypertension in 45%; hyperlipidemia in 50%
DM (diabetes = afflicted with diabetes) and %50-60 of men above 50 years of age have ED
Erection types
- Psychogenic erection
- Reflex erection
- Nocturnal erection (while sleeping at night)
Erections are provided with combination of psychogenic and reflex path in general!
Penile Erection mechanism
Erection is a complex vascular chain of events controlled by nervous, hormonal and psychogenic mechanisms.
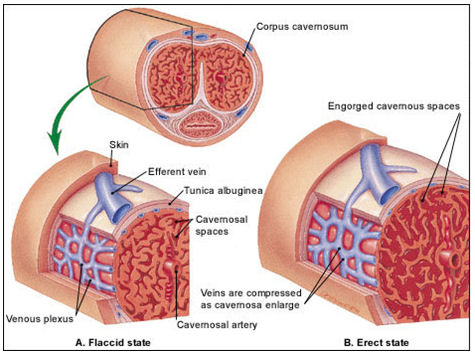
Once sexual stimulation starts (visual / tactile / spiritual), arteries entering into the penis dilates and blood flow coming is increased. Penis enlarges and extends, stores the blood within spongy structure and enters into erection. Vein system is closed to maintain erected position of the penis.
When sexual stimulus is discontinued or ejaculation occurs, system becomes reversed.
Penis Anatomy
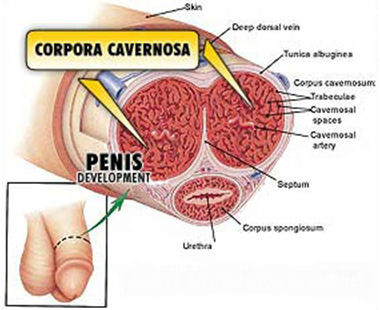
Penis consists of 2 cavernous corpus (CC) on the top, 1 spongious corpus (CS) on the nottom and glans (head).
CCs include trabecules surrounded by smooth muscle and sinusoids.
Urethra passes along CC.
CCs are covered by tunica albuginea which is poor in elsatic fibers, rich in collagen fibers with limited distensibility (enlargement capacity).
Tunica albuginea prevents venous return by compressing emissary veins which pass along during the erection as it has a limited enlargement capacity.
Contraction of ischiocavernous and bulbocavernous muscles increase the hardness, helps ejaculation.
CAUSES FOR ED
Erection problems will be experienced in case of presence of one or more of the following conditions:
- problems preventing dilatation in arteries
- Spongy structures that will restrain the blood within the penis
III. Problems of connective tissue and vein that prevent blood return

RISK FACTORS that may cause ED
- Aging
- Chronic Diseases (Atherosclerosis – Diabetes – Cardiac Diseases – renal Diseases – Liver Diseases)
- Operations and Traumas
- Drugs
- Smoking and other modifying factors
DIAGNOSIS: PATIENT EVALUATION
- Medical History
- Sexual history
- Physical Examination
- Psychological evaluation
- Laboratory tests
For an individual who refers by “erection difficulty” complaint, the following should be asked for the past 6 months period.
Status of the sexual desire
Depression – stress – anxiety disorders
Marriage problems
Work and life problems
The evaluation of the patient must be done by a specially designed questionare. The scoring system is used in evaluation of the severty of ED and later the result of the treatment. Ed can be classified as no ED, mild, mild-moderate, moderate, severe.
TO OBTAIN A GOOD ANAMNESIS
If the person;
Has spontaneous erections,
Morning erections,
Sufficient erection by masturbation,
Erection except his usual partner,
ORGANIC causes may be excluded roughly, PSYCHOGENIC cause is highly possible!!!
DIAGNOSIS FOR ORGANIC ED
Laboratory Tests
Complete Blood Count – Urea – Creatinine – Liver function tests – Blood Fats (Cholesterol- Lipids) – fasting Blood Glucose (FBG) – Total and free testosterone – Prolactin Hormone (PRL)
Intracavernous Pharmacological Testing

All agents used cause dilatation in arteries and closing in veins and blood is restrained within the penis and erection occurs. It provides information about vascular bearing of the penis. Negative response is not diagnostic. However, if almost complete erection develops within first 12 minutes following the injection and such erection continues for 30 minutes , it may be deemed that such person does not have any vascular problem.
Drugs used During Intracavernous Pharmacological Testing:
- Papaverine 15 – 60 mg
- Papaverine 30 mg/ml + Phentolamine 1 mg/ml : 0.2 – 1 ml
- Prostoglandin E1 5 – 15 microgr.
- Papaverine 12 mg + Phentolamin 1 mg + PGE1 9 micrgr : 0.1 – 0.5 ml
Color Doppler Ultrasonography Of Penis
It is useful to perform with pharmacological tests. It provides an opinion about penis anatomy and vascular bearing.
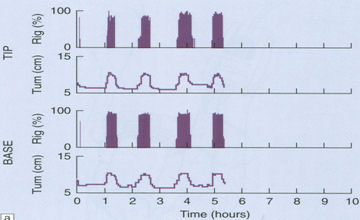
Nocturnal Penile Tumescence (NPTR) Rigiscan Monitor:
 Erektil Disfonksiyon The safest test for differentiation of organic and psychogenic ED
Erektil Disfonksiyon The safest test for differentiation of organic and psychogenic ED
It is a tool to obtain information about nocturnal erection count and quality. We obtain such information in some graphics.
(Positive response without any neurogenic or hormonal pathology (Multiple erections which may occur 3 to 6 times per night, reach to 70% hardness of normal erection and last for 10 to 15 minutes are measured) = Psychogenic)
Pharmacological cavernosometry – graphy
It is used to determina the location of venous leakage. It is useful to perform if operation is planned.
Angiography
It is important especially to detect the arterial disorder out of the penis and to determine the further operation.
It may be diagnosed with specific neurological tests.
CURRENT METHODS FOR ED TREATMENT
Non-invasive methods
Elimination of risk factors
Consultancy – Psychotherapy
Oral and topical drugs
Vacuum tools

It is an ideal and cheap method for the patients who do not consider any drug or invasive treatment. Penis is placed into a plexyglass lantern and blood flows into the penile vessels by effect of the negative pressure while the air inside is discharged. Penis enlarges and extends. A plastic ring is places into the bottom of the penis to maintain the erection and lantern is removed. The person may have an intercourse as he desires for about thirty minutes.
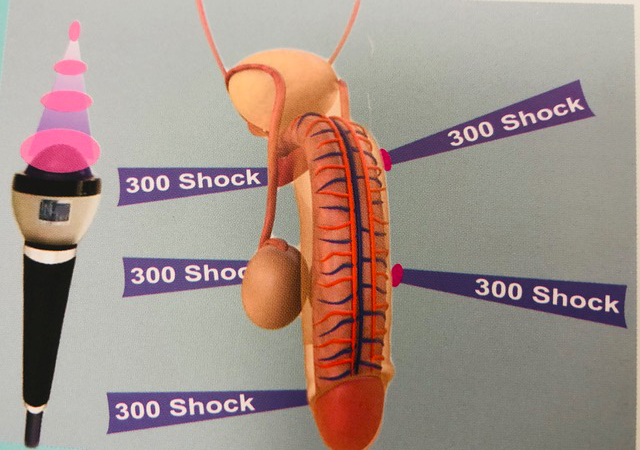
LI EDSWT:
Low Intensity Shockwave Therapy for Erectile Dysfuntion
The ED-SWT is designed to deliver extracorporeal, focused, low-intensity shockwave therapy to the penile area of patients suffering of vascular related Erectile Dysfunction (ED).
The ED1000 system is a device for Extracorporeal Shockwave therapy. It non-invasively delivers low-intensity shockwaves to specific areas in the patient penile shaft and crus consequently improving local blood perfusion in this area and improving erectile function.
The ED-SWT is intended for use as alternative/complement treatment of patients with vascular related Erectile Dysfunction.
The treatment with ED-swt is painless. In each seance shocks are delivered to 5 different areas of the penis. 300 shocks delivered to each area.
The machine produces 120 shocks per minute. The total amount of shocks per seance are 1500 and lasts about 15 minutes. In mild cases 6-12 seances; mild – moderate cases 12- 36 seances are generally enough for the treatment.
Invasive methods
Transurethral drug applications

Alprotadyl use is especially common in USA. A drug is loaded into the urethra with its special device just before the intercourse.
Intracavernous Drug Applications (Intra Cavernous Injection ICI)

Papaverine and/or prostaglandin derivates may be used single or in combination with different doses just like diagnosis step before the intercourse. A special training should be given to the person to apply this injection by himself.
Penile Prosthesis
Although it is a gold standard for ED treatment, treatment should progress from the least invasive to the most invasive.
Prosthesis use is a irreversible decision!
Prosthesis may be with single or multiple pieces.

None of the prosthesis;
provides erection just like normal physiological erection!!!
Models that can not be blown up;
Causes to keep the penis on same size and diameter all the time!
Hydraulic models;
Are expensive but more physiologic.
Diameter increase occurs during the erection!
VASCULAR SURGERY
Vascular by-passes may be applied to increase the blood flow into the penis with some microscopic techniques.
CHARACTERISTICS OF IDEAL DRUGS
Efficient – Useful – without side effects – easy to use – specific and cheap.
Some agents effecting on different locations (from the brain or penis vessels etc.) with different mechanism of actions:
papaverine – nitroglycerine – verepamil – alprostadil – phentolamine – phenoxbenzamine- yohimbin – sildenafil – tadalafil – vardenafil – apomorfin – trazadone etc.
While using these agents, to be under physician control is required. Because some serious side effects may appear. (for example, those using drugs dilating cardiac vessels such as nitrate may have fatal risks.)
DIAGNOSIS AND TREATMENT PRINCIPLE ACCORDING TO TREATMENT EXPECTATION OF THE PATIENT
- Oral Treatments / Transurethral therapies / Vacuum device
- NO TEST IS NEEDED
- ICI : Intracavernous drug injection
- ICI Test
- Penile Prosthesis
- ICI test / NPT test / Penile doppler US
- Venous surgery
- ICI test / Penile doppler US / Cavernosometry / Cavernosography
- Arterial surgery
- ICI test / Doppler US / cavernosometry / cavernosography / Pharmacoarteriography
TREATMENT FOR PREMATURE EJACULATION (EJECULATIO PRECOX)
Premature ejaculation may be defined as occurrence of the ejaculation within a short period so that parties can not obtain the required pleasure from sexual intercourse.
The basic cause depends on habits and/or psychogenic factors.
TREATMENT
- CONDOM USE
- ANESTHETIC POMADES
- SEX THERAPY
- SQUEEZING TECHNIQUE (MASTER & JOHNSON)
- MEDICAL SUPPORT
Sertraline – Fluoxetine – Clomipramine – Trazadone